Select date
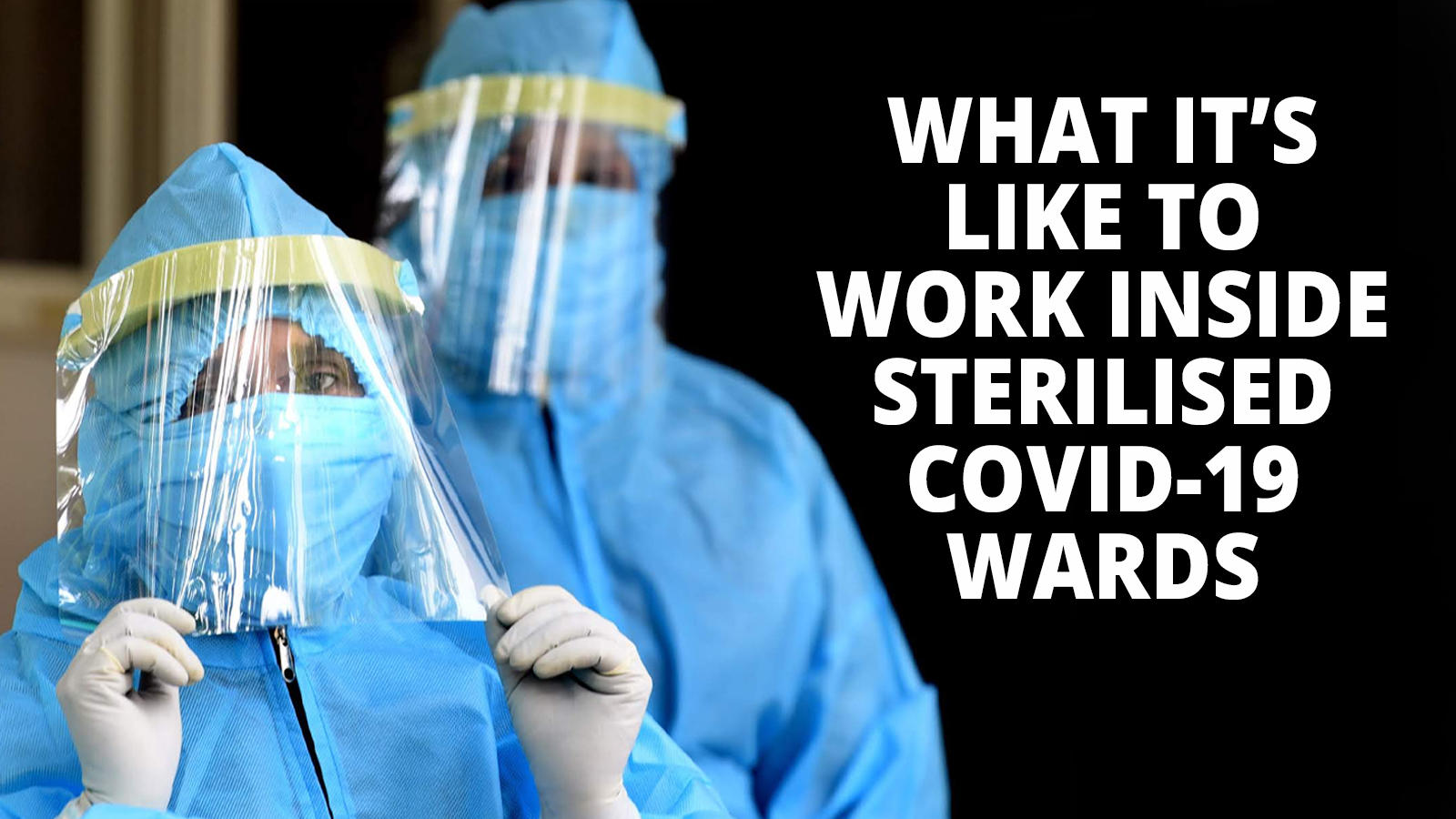
What It’s Really Like to Work in a COVID Ward


by Chuck Hudson, The Organic Prepper:
Editor’s Note: This article was written by a personal friend of mine. This isn’t some stranger who wrote to me to share some story that may or may not be true. This is a man I’ve known for years who has dedicated his entire career to caring for the health of others. In this essay, he shares an average day in the COVID ward of the hospital where he works. ~ Daisy
COVID virus has turned the world upside down. From the economy of the planet to pitting neighbor against neighbor and friend against friend. Never mind the violence destroying our cities. We are all dealing with this virus with totally unbelievable numbers, huge numbers of infected people, and a rising death toll.
Yet, I look out my living room window and see green grass, flowers blooming and some kids down the street playing basketball.
And then, I go to work.
The area where our day patients come in is called 2HVT. All 14 rooms of 2HVT are now negative pressure rooms. (Also called isolation rooms, negative pressure rooms help prevent airborne diseases from escaping the room and infecting others.) All the rooms of the old Cardiac ICU, which is attached to our cath lab by a short hall, are now negative pressure rooms. 4 South on the 4th floor is now a COVID unit. 6 south, an old Ortho ward, and 5 South have been converted as well. All these conversions are in the downtown hospital alone. All patient areas of the 3, newer hospitals in the system have been converted to handle COVID patients.
Watching the news here in my new home state of South Carolina, no matter the station, it is the same thing: doom and gloom. More and more infected people from testing, talking heads pointing the finger of blame, and numbers being sensationalized. After all, “If it bleeds it leads.” It’s gotten so bad that I turn on the news just long enough to catch the weather and traffic for the morning drive from Summerville to Charleston.
But enough of that. Let me tell you what it is really like in the COVID step-down unit. This unit is for people not sick enough to need high flow O2 or intubation, yet too sick to go to a “regular” floor. (Like there is a regular COVID floor!) As with any floor, the “permanent “ nurses and techs get morning reports from their night shift counterparts. After getting the reports we start our rounds with the patients.
Wait…no, we don’t just walk into a COVID room.
It takes about 3-5 minutes to gear up before entering a room.
Step 1 put on a set of gloves.
Step 2 Put on impermeable gown.
Step 3 Put on N95 mask.
Step 4 Put on face shield. ( We 3D print the frames for these. And use pieces of acetate we get from Staples. )
Step 6 Put on 2nd set of gloves.
Step 7 Triple check that everything is sealed and in order.
Now…we can go in the room.
We try to allow only 1 person at a time in the room, unless something demands that 2 people are needed. The nurse or tech who goes in the room does not leave the room until they have completed all tasks. If the nurse or techs needs something this is where I come in. If I am not assigned a patient, I run and get things. We are runners. We run and get whatever is needed.
What about emergencies?
Same procedure.
We have Mayday bags stapled to the wall in front of each room. Each of these Mayday bags contains the following:
- 2 N95’s: small and regular
- “Bunny Suit”
- Face shield (We 3D print face shields in-house)
- 6 pairs of separately bagged gloves (sm, med, lg)
- Bouffant hat
All of this must be put on prior to entering a room. It is mandatory. Even if the patient is dying.
Very little is talked about…so much to tell.
Even the little things that the patients and the staff endure take a huge toll on us.
A majority of our patients have lost their sense of taste and smell. Some can only sense texture and temperature. This makes it difficult and frustrating for our patients and staff. The food delivered to our COVID patients is left at the “Airlock”. In normal rooms, insulated containers can be used for the food, keeping it hot. However, food in the COVID areas must be served using only paper plates, paper cups, paper serving trays and plastic ware. We have to use a microwave to heat the food just before it goes in the room.
In normal rooms a tech, nurse or CNA brings the food to the patients. In our world, only the assigned nurse or tech brings the food. And it may be a LONG wait due to having to microwave the food just prior to going in. We have to coordinate routine care to keep the number of times a room is entered to a minimum. (I have become an expert at microwaving paper plates of hospital grade food!)
One thing the virus does that many people outside of the medical field don’t know is it interferes with the blood clotting cascade. Believe you me, as a former Medical Lab Tech (MLT) I would LOVE to go over in mind-numbing detail the 12 steps of clotting. The intrinsic and extrinsic pathway that lead to a fibrin strand…”OUCH!” (My wife just tossed a crafts magazine at me. I started describing the steps. In detail.)
So, in addition to damaging the lungs, COVID can cause deep vein thrombosis. It also causes DIC (Disseminated Intravascular Coagulation.) Post mortem exams have revealed up to 30% of early COVID patients had elevated D-Dimer, C-reactive protein and lactate dehydrogenase. All markers for clotting system problems, which has led to death by stroke, even in young people.
Some patients are in denial until the last moment.
Recently, I was helping to discharge a fairly young patient, about the mid to late 40s. As I was getting his history and gathering information on his experience, I asked how he ended up in ICU and then in my area.
He told me he thought he had a summer cold. He thought the whole virus was a hoax and refused to wear a mask. When his wife brought him in he thought it was a bad cold AND an ulcer. He complained of stomach pain, severe diarrhea, and shortness of breath. He was admitted to our COVID floor, still in denial. What he had believed was a stuffed up nose was actually him losing his sense of smell. Then he crashed.
The anesthesiologist did what is called rapid sequence intubation. The patient is given sedative and paralytic drugs. That’s it. Once they are intubated, they are put out.
He told me when they jerked his head back and he saw that the young doctor looking scared though his protective gear he knew then it wasn’t a hoax.
Good news: we ARE saving more than we lose.
Here in Charleston where I work, our average patient stay is 4 days. If they go to the ICU their stay is about double that. In the last 3 weeks we have dropped from 44% to 31% of our inpatients being in for COVID. Our percentage of positive COVID tests is at about 21%. We test EVERY PATIENT that comes in the hospital.
We have a game plan:
- Remdesivir
- Lovanox
- Plasma antibodies from COVID survivors
- Intervene and intubate
- ECMO: Extracorporeal membrane oxygenation (to treat some patients)
We have a long way to go. We still have shortages of protective gear, but we improvise, adapt and overcome. Up to 170 or so of our teammates, young and not so young, have been out with COVID. Some ended up in the ICU. Our hospital is finding ways to use senior management. A large group of nurses that haven’t been bedside in years are filling in as runners, housekeepers, and patient transport.
Read More @ TheOrganicPrepper.ca


